Pelvic floor disorders is a frequent pathology whose prevalence is estimated at between 30 and 50% of women (prolapse of all stages combined).
The organs of the three levels of the pelvis can be affected :
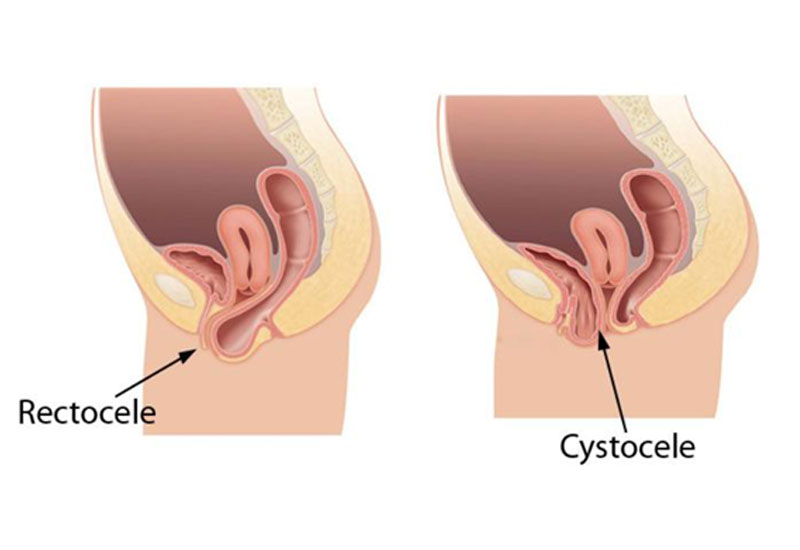
- the bladder (cystocele),
- the uterus (hysterocele),
- the rectum (rectocele).
The disorders observed are mainly of obstetrical origin (large fetus, instrumental maneuvers, prolonged labour, midline episiotomy, perineal injury). Aging, hormonal deficiency or any increase in abdominal pressure (chronic constipation, chronic cough, obesity, high-level sports activities) are also involved. A rectal prolapse can be associated or isolated to the previous disorders
A balance sheet
The associated symptomatology is variable and most often includes perineal discomfort, pelvic heaviness, more rarely pelvic pain and dyspareunia (pain felt during and/or after sexual intercourse).
Urinary or digestive symptoms may also be associated: urinary incontinence or dysuria (difficulty urinating), anal incontinence or dyschezia (difficulty passing stools), all leading to an alteration of body image.
In order to offer you the best possible strategy, your surgeon will rely on the following examinations :
- Urodynamic assessment: examination aimed at studying various parameters of the bladder and its sphincter,
- Dynamic MRI or defeco-MRI which is the exploration of the position at rest, in thrust and in restraint of the different organs (bladder, uterus, vagina and rectum),
- Anal ultrasound exmanination and manometry may be also requested.
The management
Surgical treatment of symptomatic prolapse should be based on risk/benefit analysis. This analysis is mainly based on the description of the symptoms and their impact on quality of life, the clinical examination carried out during the consultation, and complementary exams.
All case are discussed within a MDT meeting (Multi-Disciplinary Team) foussed on pelvic floor disorders involving urologists, gynecologists, digestive surgeons and radiologists.
Depending of the surgery, the operative procedure may involve 2 surgeons (digestive surgeon and gynecologist or urologist).
