
Colon cancer is the second leading cause of death in men and the third in women in France.
The main risk factors are alcohol consumption, overweight and obesity, smoking, low fiber diet with excessive consumption of red meat or processed meat, sedentary lifestyle and physical inactivity.
A family or personal history of colorectal cancer can also be a risk factor.
It is important to get tested as soon as possible to increase the chances of recovery.
This is why a screening program is offered in France to all people from 50 to 74 by looking for blood in the stool. Nevertheless, despite the prevention campaigns, the participation rate in the general population remains low and does not exceed 35%.
A balance sheet
In the event of a positive screening test and/or the appearance of symptoms (anaemia, recent transit disorder, unexplained weight loss, bleeding in the stools, etc.), your doctor will refer you to a gastroenterologist who will carry out a complete pre-therapeutic assessement with :
- A complete colonoscopy with biopsy required to confirm the diagnosis,
- A thoraco-abdominopelvic CT scan (to exclude other locations),
- A recent biological assessment (with a blood count (NFS), a nutritional assessment (albumin/pre-albumin) and the dosage of tumor markers (ACE/CA 19-9).
In the majority of cases and thanks to an early diagnosis, a team surgeon will be able to offer you the most appropriate treatment.
The management of Colon cancer
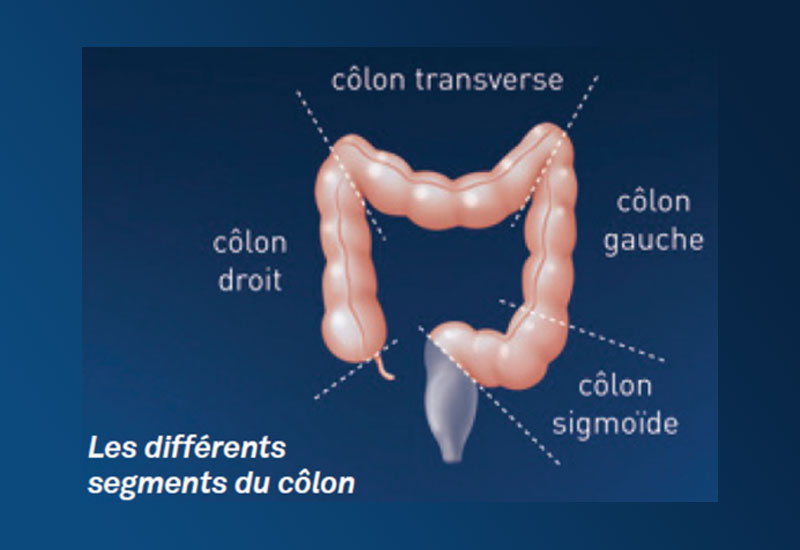
Depending on the location of the tumor in the colon, the part of the diseased (called pathological) colon is removed.
The two most frequent interventions are the right colectomy and the left colectomy (= removal of the right colon/left colon).
Colon surgeries can be performed by laparoscopy (small incisions in the abdominal wall and camera) or by robotic approach (= small incisions in the abdominal wall with robotic assistance). These techniques, called minimally invasive surgery, allow a reduction in post-operative pain compared to the open approach (= a large incision in the abdominal wall), reserved today for less than 10% of our patients.
It is exceptional to place a stoma (pouch or artificial anus) during these interventions outside of the emergency (occlusion or peritonitis on perforation of the colon).
In the absence of post-operative complications, the hospital stay is approximately 3 days. We are currently working on reducing this within a multidisciplinary professional project with a view to continuous improvement within our team.


Your Care Pathway
At the end of the consultation or during your hospitalization, the surgeon may suggest that you participate in a research protocol, such as a study evaluating a new surgical device, a new method of administering it, new surgical techniques, personalized therapeutic strategies, etc.
- Make an appointment
Online or by phone - I am preparing for my hospitalization
Your hospitalization - My exit and return home
Your return home