
Hernies et éventrations abdominales, péristomiales (autour de la stomie) et périnéales
— une expertise chirurgicale complète au service de chaque patient
Hernias and Incisional Hernias : What Are They ?
A hernia and an incisional hernia share the same underlying mechanism: an abdominal organ (such as the intestine or omentum) protrudes through a weakened area of the abdominal wall.
 |  |
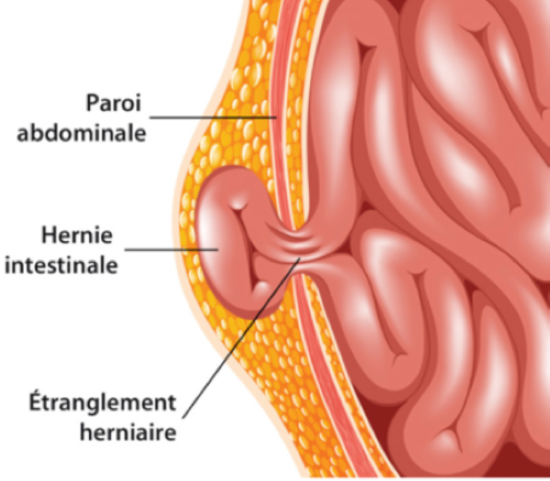
In both cases, an intra-abdominal organ bulges through a natural opening or a defect in the abdominal wall, creating a visible or palpable swelling.
This bulge may be reducible (disappearing when lying down or with gentle pressure) or irreducible. In some cases, the hernia may become strangulated, cutting off the blood supply to the trapped organ. This is a surgical emergency.
-When is surgery recommended ?
Surgery is recommended when the hernia causes symptoms (pain or discomfort), complications (strangulation or bowel obstruction), or significantly affects the patient's quality of life.
-Surgical treatment
The surgical approach is based on one of the following techniques:
- Primary repair (direct suture), generally reserved for small hernias.
- Reinforcement with a prosthetic mesh, commonly referred to as a "mesh repair."
Depending on the size of the abdominal wall defect, the type of hernia, and the patient's surgical history, the procedure may be performed using either an open or a minimally invasive (laparoscopic) approach.
PARASTOMAL HERNIA
-What is it ?
A parastomal hernia is a type of incisional hernia that develops around a stoma (colostomy or ileostomy, digestive or urinary). It occurs when the abdominal wall weakens or enlarges around the stoma opening, allowing the intestine or omentum to protrude. It is a very common complication, affecting 30–50% of patients with a stoma, and typically presents as a visible bulge around the stoma, particularly when standing or during physical exertion.
An abdominopelvic CT scan is recommended to assess the size and volume of the hernia and to identify any associated abdominal wall hernias.
-When is surgery recommended ?
- Functional symptoms: pain, discomfort, difficulty standing or walking
- Problems with stoma appliances: poor fitting, recurrent leakage
- Acute complications: strangulation (surgical emergency)
Surgical treatment of a parastomal hernia requires a comprehensive assessment of the patient's overall health, comorbidities, and symptoms, as the risk of recurrence remains significant.
-Surgical treatment
Repair generally involves reinforcement with a prosthetic mesh, positioned around the stoma to close the abdominal wall defect. Depending on the individual case, the procedure may be performed using an open or laparoscopic approach. Preoperative optimization may be required.
PERINEAL HERNIA
-What is it ?
A perineal hernia may occur following an abdominoperineal resection (APR) or total proctectomy with perineal excision (pelvic exenteration). After removal of the rectum and anal canal, abdominal organs may descend through the weakened pelvic floor into the perineal region.
It affects up to 25% of patients following APR, with a higher risk in those who have previously received pelvic radiotherapy.
An abdominopelvic CT scan helps determine the size of the perineal defect, identify its contents, and evaluate the extent of pelvic floor muscle involvement.
-Symptoms
- Painful perineal bulge, worsened by prolonged standing
- Chronic perineal heaviness or discomfort
- Acute complication: bowel obstruction due to strangulation of an intestinal loop through the perineal defect
-Surgical treatment
Treatment consists of reconstructing the pelvic floor using a prosthetic mesh. The repair may be performed through an abdominal approach (laparoscopic or robotic), a perineal approach, or a combined abdominal and perineal approach, depending on the patient's anatomy and the complexity of the hernia.