The surgical management of bowel endometriosis is provided in partnership with IFEMENDO, a recognized expert center dedicated exclusively to the treatment of endometriosis, located within Clinique Tivoli in Bordeaux. Consultations, preoperative assessment, and appointment scheduling are carried out through the IFEMENDO website.
What is bowel endometriosis?
Deep endometriosis is a condition in which tissue similar to the lining of the uterus (the endometrium) grows outside the uterus. When these lesions infiltrate the digestive tract, the condition is referred to as bowel endometriosis.
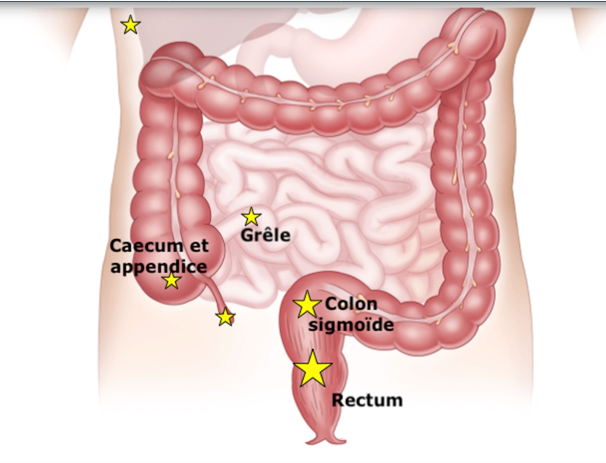
Bowel involvement is the most common non-gynecological manifestation of deep endometriosis. In the vast majority of cases, lesions are located in the rectum and sigmoid colon. Less commonly, they may affect the appendix, terminal ileum, or cecum.
Symptoms of bowel endometriosis
Symptoms are often subtle and develop gradually, sometimes remaining unnoticed for many years. They vary depending on the size and depth of the endometriotic lesions.
- Bowel habit changes: alternating diarrhea and constipation, often worsening during menstruation (catamenial symptoms).
- Dyschezia: difficulty passing stools, painful bowel movements, excessive straining, or urgency.
- Bloating and nausea: abdominal distension, nausea, and occasionally vomiting when rectal narrowing becomes significant. These symptoms may indicate an increased risk of bowel obstruction.
- Rectal bleeding: bleeding directly caused by endometriotic lesions is uncommon. In most cases, rectal bleeding is related to hemorrhoids secondary to chronic straining during defecation.